

 Menu
Menu

 Search
Search

- News

- Economy

- Central Banks
- Investing
- Research
- Roundups
- Digital Currency
- Insights
- Technical Analysis
- Technology
- Business
- Law
- Health
- Nature
- Fintech
- Science
- Topic
- Opinions
- ©Econometrics LLC . All Rights Reserved.

James Malone-Lee
I qualified from St. Thomas' Hospital, London in 1975. Having served with the Royal Army Medical Corps until 1981, I joined University College London as a lecturer in geriatric medicine, then senior lecturer in 1984. I was promoted to a personal chair in 1994 moving to the Barlow Chair of Geriatric Medicine in 1996.
In 1999 I moved to the Whittington hospital campus of the school as Professor of Medicine, Head of the Department of Medicine for that campus. My personal research work has always been on urinary incontinence but at the Whittington Hospital he has supervised a much broader brief in clinical science.
My research work has focused on the pharmacology, biomechanics and physiology of urinary incontinence. In recent years my discoveries in relation to chronic bladder inflammation in the aetiology of overactive bladder have resulted wider collaborations with microbiologists, physiologists, immunologists and pharmacologists. I am a keen supporter of basic science as the foundation of modern medicine but nevertheless I remain an avowed clinical researcher.
I can summarise my discoveries as follows:
Urodynamic investigations appear to provide little information useful to the clinical management of patients with lower urinary tract symptoms
Quantitative microbiology applied to the routine MSU, based on the Kass criteria of 1957 to 1960 is extremely insensitive, missing many genuine infections.
The dipstick tests for leucocyte esterase and nitrite are substantially worse than the culture methods. Such tests should not now be used to exclude urine infection.
Microscopy of a fresh unspun, unstained specimen of urine, to count the urinary leucocytes is the best test for urine infection that we have but it will miss about 40% of infections.
Many persons with lower urinary tract symptoms are living with chronic infections that go untreated because of contemporary guidelines.
The symptoms that patients describe are extremely important, accurate and the best guide to the pathology afoot. They should never be ignored and pain is not necessarily essential.
Many urine infections are caused by mixed colonies and mixed growths are associated with important independent markers of urinary tract inflammation and infection.
Many urine infections involve intracellular bacterial colonisation of the urothelium by mixed pathogens that are fastidious and extremely difficult to treat by conventional methods.
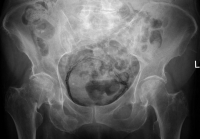
How poor NHS testing and antibiotic use is creating super-strength cystitis
Sep 20, 2016 11:50 am UTC| Health
Urinary tract infections also known as cystitis are extremely common. Around 150m people are affected worldwide each year and one in every three women is expected to suffer at least one attack before they are 24. But...

South Africa Eyes ECB Repo Lines as Inflation Eases and Rate Cuts Loom

Russian Stocks End Mixed as MOEX Index Closes Flat Amid Commodity Strength

China Extends Gold Buying Streak as Reserves Surge Despite Volatile Prices

Trump Lifts 25% Tariff on Indian Goods in Strategic U.S.–India Trade and Energy Deal

Trump Signs Executive Order Threatening 25% Tariffs on Countries Trading With Iran


New York Legalizes Medical Aid in Dying for Terminally Ill Patients

Trump Says “Very Good Talks” Underway on Russia-Ukraine War as Peace Efforts Continue

China Warns US Arms Sales to Taiwan Could Disrupt Trump’s Planned Visit

Trump Allows Commercial Fishing in Protected New England Waters

SpaceX Prioritizes Moon Mission Before Mars as Starship Development Accelerates

NASA and SpaceX Target Crew-11 Undocking From ISS Amid Medical Concern

Neuralink Plans High-Volume Brain Implant Production and Fully Automated Surgery by 2026

Jared Isaacman Confirmed as NASA Administrator, Becomes 15th Leader of U.S. Space Agency
Senate Sets December 8 Vote on Trump’s NASA Nominee Jared Isaacman
Nvidia CEO Jensen Huang Says AI Investment Boom Is Just Beginning as NVDA Shares Surge
Amazon Stock Rebounds After Earnings as $200B Capex Plan Sparks AI Spending Debate

Global PC Makers Eye Chinese Memory Chip Suppliers Amid Ongoing Supply Crunch

OpenAI Expands Enterprise AI Strategy With Major Hiring Push Ahead of New Business Offering

SoftBank Shares Slide After Arm Earnings Miss Fuels Tech Stock Sell-Off




- Market Data










